

What Is PCOS? A Melbourne Naturopath's Complete Guide to Understanding, Diagnosing, and Treating It.

Written by Jessica Diakoumakos, Naturopath (BHSc Naturopathy) · Emba Wellness, Melbourne
📌 Update — May 2026: As of 12 May 2026, polycystic ovary syndrome (PCOS) has been officially renamed polyendocrine metabolic ovarian syndrome (PMOS) in a landmark global consensus published in The Lancet. The condition itself has not changed — only its name. Both terms are used during the transition period. Read my full explainer on the PCOS to PMOS name change here.
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women of reproductive age, affecting 8–13% of Australian women — approximately 1 in 8. Despite its prevalence, PCOS is widely misunderstood, frequently misdiagnosed, and still commonly treated as a purely reproductive condition when it is, in fact, a complex metabolic, hormonal, and psychological disorder. The 2023 International Evidence-based Guideline for the Assessment and Management of PCOS — led by Australian researchers at Monash University and endorsed by major international medical bodies — identifies PCOS as a neglected, underdiagnosed condition with far-reaching implications beyond fertility, including metabolic health, cardiovascular risk, mental health, and quality of life. This post is a comprehensive guide to what PCOS actually is, how it is diagnosed under current guidelines, what is driving it, and what an evidence-based, root-cause approach to treatment looks like.
If you've been told you have PCOS — or suspect you might — you've probably also been told to lose weight, take the pill, and come back when you want to have a baby.
For most women, that's where the conversation ends.
It shouldn't be.
PCOS is one of the most complex and far-reaching conditions I see in clinical practice — and it is almost universally undertreated. Not because the treatments don't exist, but because the condition itself is rarely understood in full.
So let's change that.
What Is PCOS, Actually?
Polycystic ovary syndrome is a hormonal and metabolic disorder characterised by a cluster of features rather than a single defining cause. Despite the name, you don't need to have polycystic ovaries to have PCOS — and many women with PCOS have regular periods. This is one of the most common reasons it goes undiagnosed.
PCOS is a neglected, underdiagnosed and under-researched women's health condition that affects up to 13% of women. It is often misclassified as a reproductive disorder, despite its far-reaching implications for metabolic, psychological, and pregnancy health. PCOS is also the leading cause of infertility in women.
In Australia alone, the estimated associated healthcare costs exceed $800 million annually.
What makes PCOS particularly challenging is that it presents differently in every woman — which is why understanding your specific phenotype, your specific drivers, and your specific symptom picture is essential for effective treatment.
How Is PCOS Diagnosed?
PCOS is diagnosed using the Rotterdam criteria — an internationally recognised framework that requires at least two of the following three features to be present, after other conditions have been excluded:
1. Oligo-anovulation — irregular or absent menstrual cycles, typically defined as cycles longer than 35 days, fewer than 8 cycles per year, or absent periods altogether.
2. Hyperandrogenism — either clinical signs (acne, hirsutism, scalp hair thinning, or male-pattern hair loss) or biochemical evidence of elevated androgens on blood testing (elevated total testosterone, free testosterone, or DHEAS).
3. Polycystic ovarian morphology (PCOM) — typically identified on ultrasound, defined as 25 or more follicles per ovary or an ovarian volume greater than 10ml. Importantly, the 2023 International Evidence-based Guideline now also accepts an elevated AMH (anti-Müllerian hormone) blood test as an alternative to ultrasound for diagnosis in adult women — making diagnosis less invasive and more accessible (Teede et al., 2023).
Before confirming a diagnosis, other conditions must be excluded, including thyroid dysfunction, hyperprolactinaemia, non-classic congenital adrenal hyperplasia, and Cushing's syndrome. This is why a thorough blood panel is essential before a PCOS diagnosis is made.
Why Misdiagnosis Is So Common — And Why It Matters
I want to share something personal here, because I think it illustrates exactly why accurate PCOS diagnosis matters so much.
When I was 15, I stopped getting my period. My mother had recently passed away — I was grieving, under enormous stress, and my body was responding exactly as you would expect a 15-year-old's body to respond to that kind of trauma. My HPA axis (the stress-hormone system connecting the brain and adrenal glands) was dysregulated. My period stopped.
I was taken to a doctor. An external abdominal ultrasound was done. The ovaries appeared to have multiple follicles — which, in a 15-year-old, is entirely normal. I was told I had PCOS and that it would likely be difficult for me to have children.
I was 15. I had just lost my mother. And I was now being told I might not be able to have children.
I was put on the oral contraceptive pill to "regulate my hormones." And that was the end of the conversation.
It wasn't until I started my naturopathy degree years later that I understood what had actually happened. I never had PCOS. What I had was hypothalamic amenorrhoea — the loss of my period driven by psychological stress and grief. My body had, quite literally, shut down reproduction in response to a perceived survival threat. It was a physiologically intelligent response to an extraordinarily painful situation. It had nothing to do with PCOS.
The misdiagnosis happened because of several failures that are still common today:
An external ultrasound was used on an adolescent. The 2023 International Evidence-based Guideline explicitly states that ultrasound should not be used to diagnose PCOS in adolescents within 8 years of menarche — precisely because polycystic-appearing ovaries are normal in adolescence and cannot be used as a diagnostic feature in this age group (Teede et al., 2023).
The full clinical picture was not considered. A 15-year-old who has recently lost a parent and stopped menstruating does not need an ultrasound. She needs someone to understand that profound psychological stress activates the HPA axis, suppresses GnRH pulsatility, and can completely shut down the menstrual cycle. This is textbook hypothalamic amenorrhoea — not PCOS.
Only one criterion was technically present. Under the Rotterdam criteria, at least two of three features are required for diagnosis. Irregular cycles alone — or ovaries that appear polycystic on imaging alone — do not constitute a PCOS diagnosis.
The psychosocial context was ignored. Nobody asked how I was. Nobody connected the dots between losing my mother and losing my period. The most obvious explanation — grief-driven amenorrhoea — was never considered.
I share this not to criticise any individual clinician, but because this type of misdiagnosis is not rare. Women are over-diagnosed with PCOS based on incomplete workups, and they are under-diagnosed when their symptoms don't fit the textbook picture. Both have consequences.
Being told at 15 that you may not be able to have children is a significant thing to carry. And being put on the pill to "fix" something that never needed fixing meant that the real driver — unprocessed grief and a dysregulated nervous system — went completely unaddressed.
This is why I take PCOS diagnosis seriously, why I take a thorough history before drawing any clinical conclusions, and why I always consider what else might be driving the symptom picture before reaching for a diagnosis.
If you've been diagnosed with PCOS — especially in adolescence, or without a full blood panel — it may be worth revisiting that diagnosis with fresh eyes.

The Four Phenotypes of PCOS — What Your Diagnosis Means
One of the most important — and most overlooked — aspects of PCOS is that it exists on a spectrum. The Rotterdam criteria produce four distinct phenotypes, each with different clinical features and metabolic risks. Understanding which phenotype you have matters clinically — because the risks differ significantly between them.
Phenotype A (classic PCOS): Hyperandrogenism + anovulation + polycystic ovaries. The most common and most metabolically significant phenotype. Highest risk of insulin resistance, metabolic syndrome, and cardiovascular complications.
Phenotype B: Hyperandrogenism + anovulation, without polycystic ovaries on imaging. Carries similar metabolic risk to Phenotype A despite no ovarian morphology.
Phenotype C (ovulatory PCOS): Hyperandrogenism + polycystic ovaries, with regular ovulation. Often missed because periods are regular. Acne, hirsutism, and hair thinning are the primary presentation.
Phenotype D (non-androgenic PCOS): Anovulation + polycystic ovaries, without hyperandrogenism. The mildest metabolic risk profile, but can significantly impact fertility and cycle regularity.
The Four Functional Types of PCOS — What's Actually Driving It
Knowing your Rotterdam phenotype tells you what features are present. But for treatment purposes, what matters even more is understanding why your PCOS is happening — what underlying driver is causing it.
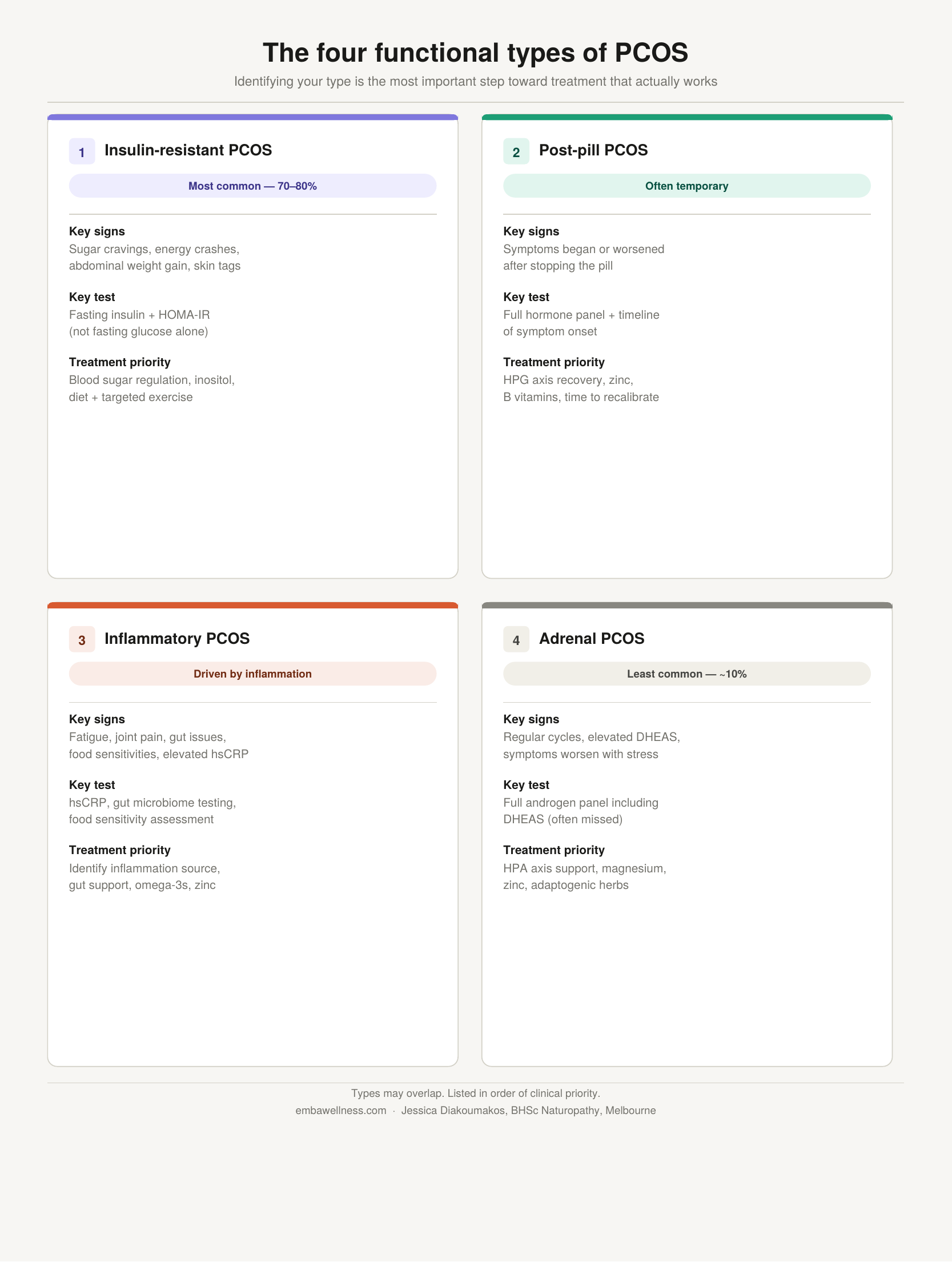
From a functional medicine perspective, PCOS can be understood as four distinct functional types, each with a different root cause and a different treatment approach. These types are not mutually exclusive — many women have overlap between them — and they are listed in order of clinical priority.
1. Insulin-Resistant PCOS — the most common type
This is the most prevalent functional type, affecting up to 70–80% of women with PCOS — including lean women (Teede et al., 2023). When cells become resistant to insulin's signal, the pancreas compensates by producing more insulin. That chronically elevated insulin — called hyperinsulinaemia — directly stimulates the ovaries to produce more testosterone and suppresses SHBG, meaning even more free testosterone circulates.
Key signs: sugar cravings, energy crashes, weight gain (especially around the abdomen), skin tags, acanthosis nigricans (darkening of skin in skin folds).
Testing: fasting insulin and HOMA-IR — not fasting glucose alone, which is frequently normal even when insulin resistance is significant.
Treatment priority: blood sugar regulation through diet, targeted exercise, and supplementation — particularly inositol, which has the strongest evidence base for insulin sensitisation in PCOS.
2. Post-Pill PCOS — often temporary
Some women develop apparent PCOS symptoms after stopping hormonal contraception — irregular cycles, acne, and elevated androgens that were suppressed while on the pill. In many cases, this is not true PCOS but a withdrawal phenomenon as the body recalibrates its own hormonal signalling.
The good news: post-pill PCOS is typically temporary, often resolving within three to six months as the HPG axis re-establishes its natural rhythm. The less good news: if it persists beyond six months, it may indicate an underlying PCOS that was masked by the pill rather than caused by stopping it.
Key signs: symptoms began or dramatically worsened after stopping the pill; no significant androgen or insulin issues prior to hormonal contraception.
Treatment priority: supporting HPG axis recovery, reducing post-pill nutrient depletion (particularly zinc and B vitamins), and giving the body adequate time to recalibrate before pursuing more aggressive interventions.
3. Inflammatory PCOS — driven by chronic inflammation
Chronic low-grade inflammation can independently drive androgen excess and anovulation, even in the absence of significant insulin resistance. Women with PCOS show consistently elevated inflammatory markers including hsCRP, IL-6, and TNF-α — even independent of obesity. Inflammation activates androgen production, impairs insulin signalling, and disrupts ovarian function.
Key signs: chronic fatigue, headaches, joint pain, skin conditions, food sensitivities, gut issues, or a history of autoimmune conditions alongside PCOS symptoms. Elevated hsCRP on blood testing.
Treatment priority: identifying and addressing the source of inflammation — this could be gut dysbiosis, food sensitivities, a chronic infection, or mast cell activation. Anti-inflammatory dietary strategies, omega-3 fatty acids, and gut microbiome support are central.
4. Adrenal PCOS — the least common type
This type accounts for approximately 10% of PCOS diagnoses and is characterised by elevated adrenal androgens — specifically DHEAS — rather than ovarian androgens. Importantly, women with adrenal PCOS often have normal testosterone and androstenedione levels and may ovulate regularly. It is an epigenetic upregulation of adrenal androgen production, often triggered or worsened by chronic stress.
Key signs: elevated DHEAS on blood testing with normal or near-normal testosterone; regular or near-regular menstrual cycles; significant stress history; symptoms worsen with acute stress.
Testing: a full androgen panel including DHEAS is essential to identify this type — it is frequently missed when only testosterone is measured.
Treatment priority: HPA axis regulation through stress management, adaptogenic herbs, magnesium, zinc, and pantothenic acid (vitamin B5) to support adrenal function.
PCOS Is Not Just a Reproductive Condition
This is perhaps the most important thing to understand — and the most significant gap in how PCOS is commonly managed.
The 2023 International Evidence-based Guideline is explicit: PCOS has far-reaching implications well beyond fertility, including:
Metabolic health. Women with PCOS have significantly elevated risk of type 2 diabetes, metabolic syndrome, and non-alcoholic fatty liver disease. These risks are present across all weight categories — not just in women with obesity.
Cardiovascular health. PCOS is associated with elevated cardiovascular risk markers including dyslipidaemia, hypertension, and endothelial dysfunction.
Mental health. This is the area I find most underaddressed in clinical practice.
In an Australian longitudinal study, the prevalence of depression was up to 27.3% in PCOS patients compared to 18.8% in the control group, and 50% for anxiety including anxiety disorders compared to 29.2% in the control group. A meta-analysis of 30 cross-sectional studies involving patients from 10 countries yielded a similar result: the risk of depressive symptoms is increased by 3.78-fold, while the risk of anxiety and anxiety disorders is increased by 5.62-fold compared to the control group.
Over the past decade, data have emerged demonstrating a high risk of concurrent mental health conditions, specifically depression and anxiety, but extending into other aspects of psychological health, including body image distress, eating disorders, and sexual dysfunction. International surveys suggest physician knowledge about the mental health associations with PCOS is poor and that patients are often dissatisfied regarding counselling-related psychological issues.
As someone with a background in both naturopathy and psychology, the mental health dimension of PCOS is something I take seriously in every clinical consultation. The psychological burden of PCOS — the body image distress, the anxiety about fertility, the shame around symptoms like acne and hair loss — is real, significant, and deserves to be treated as part of the clinical picture, not as a secondary concern.
Endometrial health. Chronic anovulation means the uterine lining is not shed regularly, which over time increases endometrial cancer risk. This is why supporting cycle regularity — whether through hormonal or non-hormonal means — is clinically important beyond fertility.
Pregnancy complications. Women with PCOS have higher rates of gestational diabetes, pre-eclampsia, and preterm birth. Optimising metabolic health before conception is essential.

What Does a Naturopathic Approach to PCOS Look Like?
The 2023 International Evidence-based Guideline recommends that lifestyle intervention — including diet, exercise, and behavioural strategies — be the first-line treatment for all women with PCOS, regardless of weight (Teede et al., 2023). This aligns exactly with naturopathic philosophy: address the root cause before reaching for pharmaceutical suppression.
Here's what that looks like in my clinical practice:
1. Functional Pathology First
Before treating anything, I need to understand what's actually driving the PCOS in this specific woman. That means going beyond the standard reproductive hormone panel and looking at:
Fasting insulin and HOMA-IR (the most sensitive markers for insulin resistance — not captured by fasting glucose alone)
Full androgen panel — total testosterone, free testosterone, DHEAS, SHBG
Full thyroid panel including Free T3, Free T4, TSH, and thyroid antibodies (thyroid dysfunction commonly coexists with PCOS and can drive similar symptoms)
hsCRP (high-sensitivity C-reactive protein) — a marker of the chronic low-grade inflammation that drives PCOS
Full iron studies including ferritin (iron deficiency is extraordinarily common in women with PCOS and profoundly affects energy and thyroid function)
AMH — both as a diagnostic tool and as a marker of ovarian reserve
Prolactin and LH:FSH ratio
This panel tells me which phenotype I'm dealing with, which drivers are dominant, and what the treatment priorities are. Without it, I'm treating in the dark.
2. Blood Sugar and Insulin Regulation
Given that insulin resistance is present in the majority of women with PCOS — and drives androgen excess directly — addressing blood sugar and insulin is almost always the first clinical priority.
This involves dietary strategies that reduce glucose load and improve insulin sensitivity, targeted supplementation (including inositol, which has the strongest evidence base for insulin sensitisation in PCOS), and lifestyle interventions including specific exercise approaches.
3. Anti-Inflammatory Diet and Lifestyle
Reducing the chronic low-grade inflammation that drives PCOS involves an anti-inflammatory dietary approach (rich in omega-3 fatty acids, polyphenols, and diverse plant fibre), optimising gut health, reducing ultra-processed food intake, and managing chronic stress — a significant driver of both inflammation and cortisol-mediated androgen excess.
4. Supporting the Gut Microbiome
Given the emerging evidence on the gut-PCOS connection, supporting microbiome diversity is now part of my standard approach to PCOS management.
5. Cycle Tracking and Symptom Mapping
For women who are ovulating but irregularly, or who have the ovulatory phenotype, cycle tracking provides invaluable clinical information. Understanding when symptoms peak, how they relate to cycle phase, and how they respond to interventions helps to refine treatment progressively.
6. Addressing Mental Health
Given the significantly elevated rates of anxiety and depression in women with PCOS, psychological support is part of every treatment plan. My background in psychology means this is always part of the conversation — not an afterthought. The 2023 International Evidence-based Guideline specifically recommends routine mental health screening for all women with PCOS (Teede et al., 2023).
7. Herbal Medicine
Several herbal medicines have evidence for specific aspects of PCOS management including adrenal and androgen modulation, insulin sensitisation, ovarian support, and cycle regulation. These are used in a targeted, evidence-informed way based on the individual's specific phenotype and dominant drivers — not as a generic "PCOS formula."
“I was misdiagnosed with PCOS at 15, after losing my mother. It wasn’t until I started my naturopathy degree that I understood what had actually happened — I had hypothalamic amenorrhoea, driven by grief. That experience fundamentally shaped how I approach PCOS in practice: with a thorough history, a full clinical picture, and the understanding that the most obvious diagnosis is not always the right one”
What PCOS Is Not
Because so much misinformation exists around PCOS, it's worth being explicit:
PCOS is not caused by being overweight. Insulin resistance and PCOS drive weight gain — not the other way around. Lean women get PCOS too, and weight-centric treatment approaches often miss the underlying drivers entirely. And importantly — PCOS is not one single condition with one single cause. The treatment that works for insulin-resistant PCOS will not work for adrenal PCOS. Identifying your functional type is the most important step toward treatment that actually works.
PCOS is not just a fertility problem. It has metabolic, cardiovascular, psychological, and endometrial implications that persist regardless of whether fertility is a goal.
PCOS is not something you just "manage" with the pill. The oral contraceptive pill suppresses symptoms — it does not treat the underlying condition. When the pill is stopped, PCOS symptoms typically return, often intensified.
PCOS symptoms are not something you have to live with. With the right approach — addressing the actual drivers of your specific phenotype — significant improvement is achievable for most women.
Frequently Asked Questions
-
Polycystic ovary syndrome (PCOS) is the most common hormonal disorder in women of reproductive age, affecting 8–13% of Australian women. It is characterised by a combination of features including irregular cycles, elevated androgens (male hormones), and polycystic ovarian morphology on imaging or elevated AMH. PCOS has significant metabolic, psychological, and reproductive implications beyond its effects on fertility.
-
PCOS is diagnosed using the Rotterdam criteria, requiring at least two of three features: oligo-anovulation (irregular or absent periods), hyperandrogenism (clinical or biochemical), and polycystic ovarian morphology on ultrasound or elevated AMH on blood testing. Other conditions must be excluded first. The 2023 International Evidence-based Guideline updated diagnostic criteria to accept AMH as an alternative to ultrasound, making diagnosis more accessible.
-
Yes. Women with Phenotype C PCOS (hyperandrogenism and polycystic ovaries, with regular ovulation) have regular periods but still have PCOS. Symptoms like acne, hirsutism, and scalp hair thinning may be the primary presentation. This is one of the most commonly missed presentations of PCOS.
-
From a functional medicine perspective, PCOS can be driven by four different root causes: insulin resistance (the most common, affecting up to 70–80% of women with PCOS), post-pill hormonal recalibration (often temporary), chronic low-grade inflammation, and adrenal androgen excess (affecting approximately 10% of women with PCOS). Identifying which functional type — or combination of types — is driving your PCOS is essential for targeted, effective treatment.
-
Insulin resistance is present in up to 70–80% of women with PCOS and is one of the most significant drivers — but it is not the sole cause. It drives androgen excess, suppresses ovulation, and worsens most PCOS symptoms. Addressing insulin resistance is central to naturopathic PCOS management.
-
Yes — lifestyle intervention including dietary changes, exercise, and targeted supplementation is recommended as first-line treatment in the 2023 International Evidence-based Guideline for PCOS. Many women achieve significant symptom improvement through naturopathic approaches addressing the underlying drivers of their specific PCOS phenotype.
-
The reproductive features of PCOS (irregular cycles, anovulation) resolve after menopause. However, the metabolic features — including insulin resistance, cardiovascular risk, and metabolic syndrome risk — persist and may worsen without appropriate management.
-
Yes — PCOS is both over-diagnosed and under-diagnosed. Over-diagnosis commonly occurs when a diagnosis is made based on ultrasound findings alone (particularly in adolescents, where polycystic-appearing ovaries are normal), or without excluding other conditions. Under-diagnosis occurs when women have regular periods but still have hyperandrogenism and polycystic ovarian morphology (Phenotype C). Conditions commonly confused with PCOS include hypothalamic amenorrhoea (often driven by stress, under-eating, or excessive exercise), thyroid dysfunction, hyperprolactinaemia, and non-classic congenital adrenal hyperplasia. A full clinical history and comprehensive blood panel are essential for accurate diagnosis.
-
Yes — naturopathic medicine is well-positioned to address PCOS because it focuses on identifying and treating the underlying drivers rather than suppressing symptoms. Key naturopathic approaches include functional pathology testing, insulin sensitisation, anti-inflammatory dietary and lifestyle strategies, gut microbiome support, herbal medicine, and integrated mental health support.
WANT SUPPORT WITH YOUR PCOS?
If you've been diagnosed with PCOS — or suspect you might have it — and you want to understand what's actually driving your symptoms and what you can do about it, I'd love to work with you.
At Emba Wellness, I take a comprehensive, root-cause approach to PCOS — beginning with functional pathology that tells me exactly which drivers are dominant for you, and building a treatment plan around your specific phenotype and health goals.
I offer 1:1 consultations in Melbourne and telehealth naturopathy appointments across Australia.

About the Author
Jessica Diakoumakos | BHSc Naturopathy & BHSc Psychology Clinical Naturopath & Founder, Emba Wellness — Melbourne, Victoria, Australia
Jess is a Melbourne-based clinical naturopath and founder of Emba Wellness.
She specialises in:
Gut health — IBS, SIBO, bloating, microbiome repair, leaky gut
Hormonal health — PCOS, endometriosis, PMS, perimenopause, post-pill recovery
Functional pathology — interpreting blood tests through a root-cause lens
Energy & thyroid — Hashimoto's, fatigue, burnout, adrenal dysregulation
Immune health — autoimmune conditions, chronic inflammation, immune dysregulation
Her approach is evidence-based and deeply personal. Having managed her own Hashimoto's thyroiditis through naturopathic medicine, Jess understands first-hand what it feels like to be dismissed by conventional medicine — and what it feels like to finally get answers.
Emba Wellness offers naturopathy consultations via Telehealth, across Australia.
-
Teede, H. J., Tay, C. T., Laven, J. J. E., Dokras, A., Moran, L. J., Piltonen, T. T., Costello, M. F., Boivin, J., Redman, L. M., Boyle, J. A., Norman, R. J., Mousa, A., & Joham, A. E. (2023). Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Journal of Clinical Endocrinology & Metabolism, 108(10), 2447–2469. https://doi.org/10.1210/clinem/dgad463
Tay, C. T., Loxton, D., Bahri Khomami, M., Teede, H., Harrison, C. L., & Joham, A. E. (2023). High prevalence of medical conditions and unhealthy lifestyle behaviours in women with PCOS during preconception: findings from the Australian Longitudinal Study on Women's Health. Human Reproduction, 38(11), 2267–2276. https://doi.org/10.1093/humrep/dead190
Ye, W., Xie, T., Song, Y., & Zhou, L. (2023). Insulin resistance in polycystic ovary syndrome across various tissues: an updated review of pathogenesis, evaluation, and treatment. Journal of Ovarian Research, 16(1), 9. https://doi.org/10.1186/s13048-022-01091-0
Dokras, A., Stener-Victorin, E., Yildiz, B. O., Li, R., Ottey, S., Shah, D., Epperson, N., & Teede, H. (2024). Management of polycystic ovary syndrome must include assessment and treatment of mental health symptoms. Fertility and Sterility, 121(4), 573–578. https://doi.org/10.1016/j.fertnstert.2024.01.009
All content published on the Emba Wellness blog is written by Jessica Diakoumakos and is intended for educational purposes only. It does not constitute medical advice. Please consult a qualified health practitioner before making changes to your health care.